The marketing science of Lipitor
Until recently, statins were the most profitable class of drugs in the history of medicine, and the most profitable of them all has been Lipitor (Atorvastatin), manufactured by Pfizer.
Here is a USA Lipitor advertisement from the early 2000’s highlighting that, in patients with multiple risk factors for heart disease, Lipitor reduces the risk of heart attack by 36%. That’s an impressive reduction and one sure to be taken seriously.
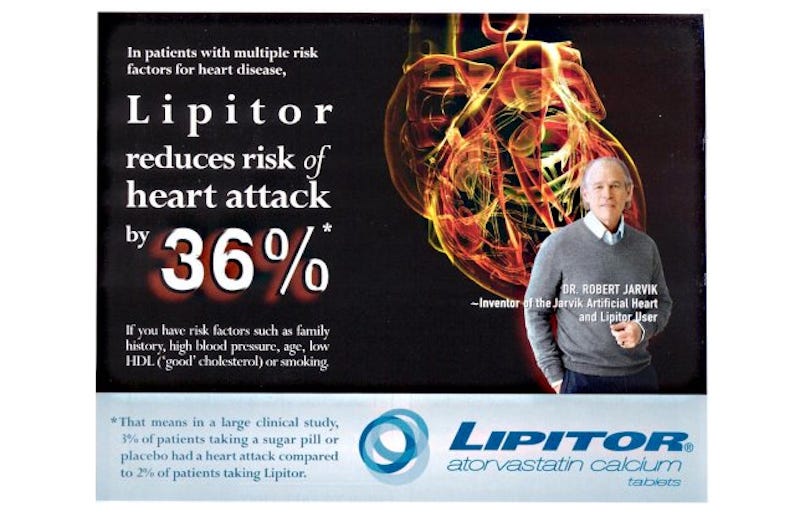
However, notice the little * after 36%. It refers to a footnote in the bottom left of the image. It’s written in blue on a light blue background, and may not reproduce well in print (especially newsprint or posters). The text is: “That means in a large clinical study, 3% of patients taking a sugar pill or placebo had a heart attack compared to 2% of patients taking Lipitor.”
Where did these numbers come from?
They come from a randomised control trial (RCT) that went under the acronym ASCOT-LLA. An RCT is the gold-standard in medical research. The trial commenced in 1998 and the results were published in 2003. The trial was stopped prematurely (after ~3.3 years of a planned 5 years) because, in the eyes of the investigators, Lipitor was showing an unequivocal benefit (when expressed in a certain way — that’s where the 36% comes in). Lipitor was already a somewhat more-effective cholesterol-lowering drug at the time, and the additional effusive press that the trial received, from sections of the medical and scientific profession and the broader media, further propelled Lipitor into orbit. For some years, Lipitor contributed up to 25% of Pfizer’s annual revenue and, overall, has achieved sales well in excess of $100 billion for the company.
Pfizer funded this RCT. Furthermore, Pfizer is the exclusive custodian of the data generated by the trial and has declined to release de-identified data for independent analysis. So, we have only the published paper to work with.
The ASCOT-LLA paper
The peer-reviewed paper reporting the results of this trial had the clumsy title: “Prevention of coronary and stroke events with atorvastatin in hypertensive patients who have average or lower-than-average cholesterol concentrations, in the Anglo-Scandinavian Cardiac Outcomes Trial-Lipid Lowering Arm (ASCOT-LLA): a multicentre randomised controlled trial.” It can be accessed online here.
Notice that the title contains: “patients who have average or lower-than-average cholesterol concentrations”. The trial was not directed at people with high cholesterol, presumably because they were already taking the drug. A successful outcome for this trial would expand the market for Lipitor to incorporate those with lower-cholesterol levels (or even independent of cholesterol levels). It is more cost-effective to expand a market for a drug than to bring a new drug to market. A later study, also funded by Pfizer, reported a benefit with high-dose Lipitor (80mg vs. 10mg) — another way to expand sales.
As well, the trial did not recruit people with a previous heart attack — this was a primary prevention trial (reducing the risk of a 1st heart attack). Therefore, success with this trial would further expand the market to incorporate people who don’t have heart disease, just risk-factors for it.
The trial was a “Lipid Lowering Arm” (LLA) carried out in “hypertensive patients”. The primary study (ASCOT) was a comparison of two Pfizer anti-hypertensive drugs. A subset of these patients was recruited into the LLA to receive Lipitor or placebo. Thus, everyone was on a blood-pressure-lowering drug, with or without Lipitor. It may seem like a confound, but Pfizer gets to sell both an anti-hypertensive drug and Lipitor this way (and it conveniently makes just such a pill).
Inclusion criteria
The ASCOT trial recruited 19,342 hypertensive patients (systolic blood pressure > 160 mmHg) without a history of heart disease (but curiously, a previous stroke or transient ischaemic attack was allowed). Participants were from family practices in the UK, Ireland and several Nordic countries. Of these, a subset of 10,305 people was identified who had cholesterol (total) concentrations of less than or equal to 6.5 mmol/L and who had at least three additional risk-factors for heart disease. These people were randomly assigned 10mg Lipitor or placebo, in addition to their antihypertensive drug. The LLA participants were almost entirely white (95%) and male (81%), with a mean age of 63+/-8 years. The trial duration was ~3.3 years (see later).
The primary endpoints
The primary endpoint is used to define and evaluate the effectiveness of a drug in a RCT. In this case, it was the occurrence of either a fatal, non-fatal, or silent heart attack (HA). A silent HA is one in which the individual does not experience symptoms, or experiences mild, atypical symptoms. In the present study, silent events were identified by electrocardiogram. There were various secondary measures, and sub-analyses performed.
The main reason for combining multiple endpoints in a RCT is to increase statistical power by detecting more events over the duration of the trial. A non-fatal HA is a major risk factor for a future attack, and silent HAs are associated with a similar level of risk, so combining these with fatal HA doesn’t seem unreasonable. However, a patient may not see it that way, and consider a fatality to be their primary concern, in which case multiple endpoints can be misleading.
For example, a number of more recent trials include revascularisation events (most commonly, operations to insert a stent). The problem arises when a reduction in the number of stents biases the difference in primary endpoint between statin and placebo, while there is a lesser (or no) difference in fatal HAs. If a person decides to take a statin to avoid a fatal HA, then the trial will be misleading for that person.
Furthermore, the media surrounding statins, whether medical or drug company sourced, speaks in emotive terms about lives saved or lost by statins, not about fewer stents.
Results
1. Cholesterol
Lipitor lowered total cholesterol (TC) and low-density lipoprotein cholesterol by about 1 mmol/L (39 mg/dl), relative to placebo, at the study end-point. This is around the expected degree of reduction for statins. It seems a little underwhelming though — a person with TC of 6 mmol/L at study entry would still have been at 5 mmol/L after ~3 years on Lipitor. Still, it could have a clinical effect over time, and that is what this trial is about.
2. Primary endpoint
The combination of all three primary endpoints yielded 100 events in the Lipitor group vs. 154 in the placebo group (the bulk of the events were non-fatal HAs). This difference was statistically significant (meaning it would not be expected to occur by chance). There were about 5,000 patients in each group. This means that around 1.9% of the people in the Lipitor group experiencing a primary event over the duration of the study. For the placebo group, this was 3.0 %.
There are three ways to represent these data.
i) Relative reduction (RR). Untreated, 3.0% suffered an event. This reduced by 1.1% with Lipitor (3.0–1.9 = 1.1). Thus the RR, expressed as a percent-reduction, is 1.1/3 x100 = ~36%. This enables the claim that: “In patients with multiple risk factors for heart disease, Lipitor reduces the risk of heart attack by 36%”. This number is not incorrect, but it is misleading without a context. There wasn’t a context in the Pfizer advertisement.
ii) Absolute reduction (AR). This is the actual difference between 3.0 and 1.9, which is 1.1%. This is a more realistic way to present the results, given that the percentages of primary events are so small overall. Thus, the claim would have read: “In patients with multiple risk factors for heart disease, Lipitor reduces the risk of heart attack by 1.1%”.
iii) Number needed to treat (NNT). This is the number of people that would need to be treated with Lipitor in order that one person would benefit. If we round the AR to 1% for simplicity, this means that 100 people would have to take Lipitor (for around 3 years) in order that 1 person benefits. In other words, 99% of people taking Lipitor will have the same outcome as if they didn’t — they either weren’t going to suffer a heart attack anyway (97%), or they suffered a heart attack despite taking Lipitor (2%).
The number needed to harm (NNH) is also important (how many people take the drug before 1 person is harmed by ‘side-effects’). Insufficient data is provided in the paper to make that calculation possible — adverse effects are barely mentioned. Drug-funded trials have an incentive to downplay harmful events associated with statins. Nearly all statin trials have been drug-funded.
Here’s how the Pfizer advertisement could have looked, using AR:

In that context, the blue text at the bottom makes more sense now. The advertisement should have also made it clear that people taking Lipitor don’t live any longer than those who don’t (see later), and that for 99 out of 100 people taking Lipitor, the outcome will be the same as if they didn’t. A more correct lead-in sentence would be: “For men with multiple risk factors for heart disease”.
3. Secondary analysis
i) There was no significant difference in all-cause mortality between groups. That is death from any cause. The majority (by far) of other statin trials also do not find a reduction in all-cause mortality, regardless of their primary endpoint findings. Thus, people don’t live longer by taking a statin, they just die from something else that may have been exacerbated by the statin. The advantage of all-cause mortality as a primary outcome measure is that it takes into account both beneficial and adverse effects on mortality. I am not aware of any study that used all-cause mortality as the primary endpoint.
ii) The numerical data for silent HA was stated in the paper — there were 14 silent HAs in the Lipitor group and 17 in the placebo group (not a statistically significant difference, the numbers are too small). However, data for the number of fatal HAs was not stated. While fatal HAs were not a stand-alone primary endpoint, they are a secondary endpoint of importance to patients, and the omission of these data is disturbing.
However, according to a document on the US FDA website commenting on this trial (as part of the Pfizer application process), there were 40 fatal HAs in the Lipitor group, and 46 in the placebo group.
Thus, fatal HAs occurred in 0.92% of people taking a placebo, and in 0.8% taking Lipitor. This gives a RR for fatal HA of 13%, and an AR of 0.12%. Based on these figures, the NNT to avoid one fatal HA would be 800. That’s 800 high-risk people to benefit one. It is also worth reflecting that in these high-risk individuals, the percentage of fatal HAs was only 0.92% over a three year period.
4. Other issues
i) The percentage values for the primary endpoint, i.e. 3.0% vs. 1.9% (placebo vs. Lipitor), were not stated in the text of the Results section or discussed elsewhere in the paper. It took a while to find them — they are in parentheses in Table 3. Furthermore, Figure 2 contradicts these values — the figure indicates they were 3.3% vs. 2.1% (which is still a RR of 36%). This sort of inconsistency is not acceptable in a publication at this level.
ii) There was no significant difference between Lipitor and placebo in women (there were few women in the trial). Women are usually under-represented in statin RCTs. The WOSCOPS trial didn’t even recruit women. There are various reasons why statins could have different effects in men and women. The Pfizer advertisement makes no distinction, presumably because women make up half the potential market.
Early termination
The study was meant to go for 5 years, but it was terminated early (median follow-up 3.3 years). This is highly problematical. There are certainly grounds for terminating a RCT early, such as an accumulation of serious adverse effects, or what is known as futility (i.e. even with continuation, a statistically significant result could not be achieved). However, stopping a study when you have got the result you are looking for is not one of them because it introduces strong bias. It is surprising that they got away with this.
The authors have the following to say: “On Sept 2, 2002, the data safety monitoring board recommended that the lipid-lowering arm of the trial be stopped on the grounds that atorvastatin had resulted in a highly significant reduction in the primary endpoint of CHD events compared with placebo and a significant reduction in the incidence of stroke. This recommendation was ratified by the steering committee”.
Three things to note: (1) It wasn’t highly significant in the common usage of the word ‘significant’, it was 1.1%. It was only highly significant statistically (p=0.0005) (2) the study did not report a significant reduction (by their own criterion, p<0.01) in the incidence of stroke, only a trend that may have gone away (or strengthened) if the study had been continued. (3) Two Pfizer employees were on the steering committee that ratified the decision to terminate. Which brings us to conflicts of interest.
Conflicts of Interest (COI)
The ASCOT-LLA involved a significant number of investigators, family practice recruitment and treatment centres, and countries. However, fourteen authors took responsibility for the analysis and publication of the data from the LLA.
There were various committees set up to enable and monitor the study, the most important of which was the seventeen-member steering committee that determined the direction of the research. All of the fourteen authors sat on this committee. Two unspecified Pfizer employees also sat on the committee. These employees did not have voting rights, but they were well placed to exert behind-the-door influence on behalf of the funding body. That leaves one lonely member, presumably carefully chosen. COIs for the data safety monitoring board were not revealed.
All authors had ties with statin (lipid) pharmaceutical companies. Their COI statement acknowledges that they “… have served as consultants to and received travel expenses, payment for speaking at meetings, or funding for research from pharmaceutical companies marketing lipid-lowering drugs, including Merck Sharp and Dohme, Bristol-Myers Squibb, Astra-Zeneca, Sanofi, Schering, Servier, Pharmacia, Bayer, Novartis, Aventis Pfizer.”
Further, it is acknowledged that all authors “… received financial support from Pfizer to cover administrative and staffing costs of ASCOT, and travel, accommodation expenses or both incurred by attending relevant meetings.”
Some final notes
There is nothing unusual about this study, how it was written-up scientifically, how it was portrayed in the media or how it was presented to the public. It could be a template.
Pfizer didn’t invent Lipitor. The company that did, approached Pfizer partly because of Pfizer’s unrivalled marketing reputation (and partly to fund clinical testing). Later, Pfizer bought out the company to prevent any of its rivals doing so.
Lipitor is now out of patent, but still making around $1 billion a year for Pfizer. The company is actively expanding its market into China, where it retains patent rights for now. I am not aware of any Lipitor study that has tested Lipitor’s efficacy in a Chinese population.
There are many other important aspects to the statin story that are not included here. My intent was to drill down into the details of this one story because of its role in supporting Lipitor’s reach into primary prevention (now normal practice).
Some questions that remain include: what do statin trials show overall and how were they funded; what happened after new RCT regulations came into force in 2005/6 in the US and Europe; what is the Cholesterol Treatment Trialists collaboration and why are they controversial; what are the real adverse effects of statins; what role do medical journals and the peer-review process play; who sets cholesterol and statin Guidelines for medical practice, and what are their COIs; what is a Risk Calculator and what is it based on; what is the evidence that high cholesterol even causes heart disease.
Disclaimer: I am not a medical doctor. Nothing herein is, nor should be taken to be, medical advice.
Further reading:
Diamond and Ravnskov (2015) How statistical deception created the appearance that statins are safe and effective.
Demasi (2018) Statin wars: have we been misled about the evidence?
